
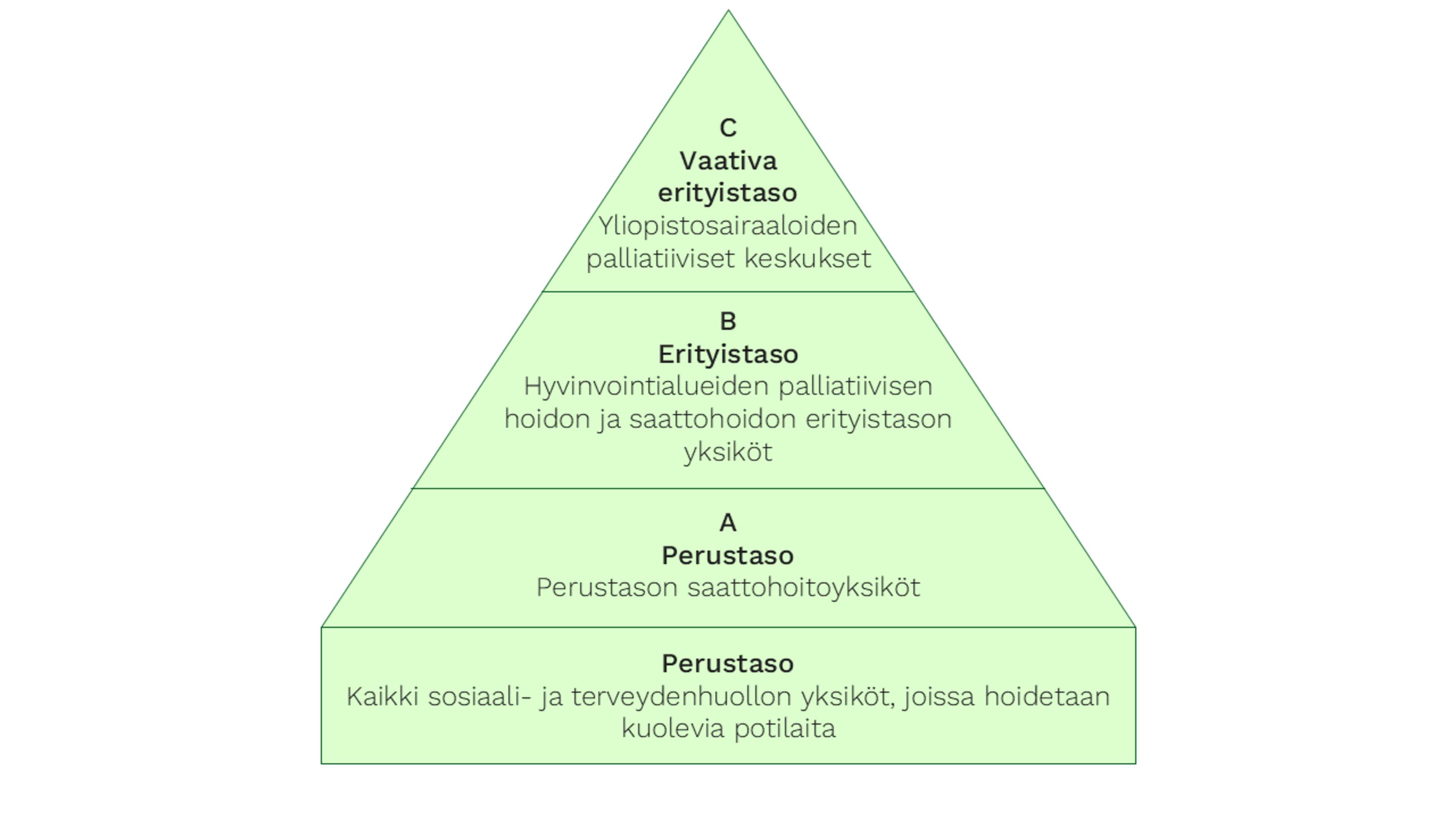
Palliative care is organised into tiers based on the patient’s needs, and integrated into the current healthcare system. The services are divided into “basic level” competence, as well as three tiers:
A – hospice care units at the basic level
B – special level palliative care and hospice care centres
C – demanding special level palliative centres.
Some wellbeing services counties have already adopted the model.
Competence of professionals
Palliative care and hospice care competence is a part of the basic skills of every social welfare and healthcare professional. According to recommendations by the Ministry of Social Affairs and Health, social welfare and healthcare professionals will have more palliative care and hospice care competence in the future, in order to provide appropriate, high-quality care in all healthcare and social welfare units. The aim is to ensure competent palliative care and hospice care equally to all those who need it, regardless of where they live..
Tiers of care
In the three-tiered model, palliative care and hospice care services are built on the foundation formed by basic-level services.